Generalization in Times of Crisis
Author: Jaime Rus Alba
 Applied Behavior Analysis is mostly implemented within controlled environments (schools, clinics, hospitals and residential settings), with a recommended 30-40 hour/week treatment plan. For services performed within a client’s home, the issue of reaching generalization in the natural environment is not so prominent, but we are still presented with the challenge of transferring stimulus control to the caregivers. Considering a time of crisis where face-to-face interventions are not possible, telehealth presents itself as the best next alternative. It is understood that many of the target behaviors within a client’s Behavior Intervention Plan (BIP) will be hardly possible to implement under a health or safety crisis such as the ongoing COVID-19 one, but not all is lost. This scenario can also be seen as an opportunity to improve our science through the assessment of generalization at home!
Applied Behavior Analysis is mostly implemented within controlled environments (schools, clinics, hospitals and residential settings), with a recommended 30-40 hour/week treatment plan. For services performed within a client’s home, the issue of reaching generalization in the natural environment is not so prominent, but we are still presented with the challenge of transferring stimulus control to the caregivers. Considering a time of crisis where face-to-face interventions are not possible, telehealth presents itself as the best next alternative. It is understood that many of the target behaviors within a client’s Behavior Intervention Plan (BIP) will be hardly possible to implement under a health or safety crisis such as the ongoing COVID-19 one, but not all is lost. This scenario can also be seen as an opportunity to improve our science through the assessment of generalization at home!
Generality was defined by Stokes and Baer (1977) as “The occurrence of relevant behavior under different nontraining conditions (i.e., across subjects, settings, people, behaviors, and/or time) without the scheduling of the same events in those conditions as has been scheduled in the training conditions.”
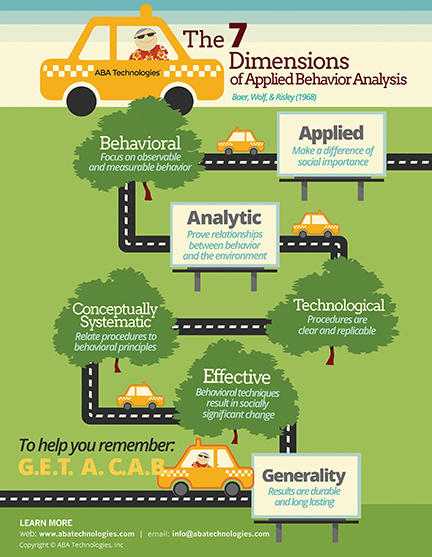 Generalization post-treatment has long been assumed rather than assessed. As one of The 7 dimensions of Behavior Analysis (Generality, Effective, Technological, Applied, Conceptually Systematic, Analytic, Behavioral), it should be present in each and every intervention developed by behavior analysts. Considering times of natural crisis (hurricanes, pandemics, floods . . . ), this post intends to transform these situations into opportunities for our clients.
Generalization post-treatment has long been assumed rather than assessed. As one of The 7 dimensions of Behavior Analysis (Generality, Effective, Technological, Applied, Conceptually Systematic, Analytic, Behavioral), it should be present in each and every intervention developed by behavior analysts. Considering times of natural crisis (hurricanes, pandemics, floods . . . ), this post intends to transform these situations into opportunities for our clients.
While much of generalization is assessed across people or settings within the controlled environment where skills are initially taught (clinic, school . . . ), a deficit exists in terms of generalization in the natural environment, specifically in the home setting as the environment to target, and with caregivers as the people to target, which the addresses as a component of “Essential Practice Elements of ABA.” Several advantages result from the correct implementation of a system that seeks in-home generalization in times of crisis:
- Generalization across people and settings will be assessed, which will give behavior analysts information on their Behavior Intervention Plan’s adherence to the dimension of generality.
- Caregivers will be included in the empirical process of behavior change, which could further develop into appropriate implementation of behavioral procedures once services are terminated.
- Supervision among BCBAs, BCaBAs and RBTs® will be able to continue, contributing to the professional development of those involved.
- RBTs®, BCaBAs® and BCBAs® will be able to bill for their services, which would reduce the economic impact of a crisis.
This fourth point sheds light on one of the most predominant factors when it comes down to approving the implementation of services: money. While being a side factor to a science, it still represents a great impact, and it is our duty to manage it in the best way possible, which would undoubtedly have a repercussion on the quality of services provided. It is important to remark that this economic impact would not only affect the providers, but also the stakeholders of ABA service.
Compliance and improvement of systems for generalization assessment might have a pivotal impact in our science and those affected by it, making challenging situations where clients are exposed to new people and environments a greater opportunity for the implementation and supervision of Behavior Analysis. Practitioners, let’s take on the challenge of generalizing our service-providing skills!
This blog contemplates two ways of addressing this opportunity:
- Retrieve targets that have reached the “mastered criteria,” as well as the “generalized” criteria within a BIP. Within these targets, select the ones that are easier to observe the client performing within the home environment (through telehealth). Arrange for environmental manipulations that could evoke these behaviors and assess for generalization! The collaboration of caregivers in order to arrange environmental-manipulation elements would be needed. Probe data could be graphed.
- Conduct Behavior Skills Training (BST) with caregivers on skills that are in the client’s current repertoire. These skills could be either “mastered” or under “ongoing treatment.” Either way, the model of BST (described in the next paragraph) will be followed. Assuming that a crisis situation in which we decide to assess generalization involves different people and a different setting than the ones provided when regular ABA services are provided, we can plan for these environmental variables to play in our favor! If the target is mastered, we can observe (through telehealth) if the client truly engages in the behavior in the presence of non-therapists (across people) and in a setting other than the clinic/school (across settings). If the target is under “ongoing treatment,” we could plan for the caregiver to gain stimulus control, therefore facilitating generalization once the target is mastered. This might seem like a lot, but you can do it!
 Behavior Skills Training is a tool commonly used within Applied Behavior Analysis, composed of a series of 4 steps: Instructions, Modeling, Rehearsal and Feedback. “A number of studies have shown behavioral-skills training (BST), instruction, modeling, role-play (rehearsal), and feedback to be used to effectively teach staff to conduct a variety of behavior procedures” (Iwata et al. 2000; Rose 2008; Roscoe, Fisher, Glover 2006). By using BST, we can assess caregivers' potential to implement behavioral procedures, as well as shaping their accuracy and reliability levels. These advantages are added to the idea of “making caregivers part of the process,” where support will be provided from a behavior analytic point of view. To perform BST in a way that benefits our clients, the following steps are suggested:
Behavior Skills Training is a tool commonly used within Applied Behavior Analysis, composed of a series of 4 steps: Instructions, Modeling, Rehearsal and Feedback. “A number of studies have shown behavioral-skills training (BST), instruction, modeling, role-play (rehearsal), and feedback to be used to effectively teach staff to conduct a variety of behavior procedures” (Iwata et al. 2000; Rose 2008; Roscoe, Fisher, Glover 2006). By using BST, we can assess caregivers' potential to implement behavioral procedures, as well as shaping their accuracy and reliability levels. These advantages are added to the idea of “making caregivers part of the process,” where support will be provided from a behavior analytic point of view. To perform BST in a way that benefits our clients, the following steps are suggested:
- Task list based on the chosen target behavior is developed by the Board Certified Behavior Analyst (BCBA). It is suggested that caregivers along with their BCBA choose which behavior will be feasible to use for the procedure. It could be helpful to take into account the physical environment where the behavior will take place, caregiver’s physical capacity to perform error correction, and the range of the video camera, for example.
- Caregivers will undergo Instruction, Modeling, Rehearsal and Feedback.
- Once caregivers are ready to perform the task, they will be evaluated on the initial task analysis developed by the BCBA on the targeted behavior.
- The BCBA/BCaBA will provide feedback on the performance.
It’s time to take a mental break. Think about how much we care for our clients!
It is important to note that procedures do not necessarily have to be implemented as they were initially written, but rather adapted to the client’s progress and the caregiver’s abilities. If caregivers implement the procedure up to mastery criteria levels after BST, three possibilities arise:
- Caregivers implement the procedure with the clients while being watched by a BCBA/BCaBA. The Analyst will only be assessing the performance of the client, which will be representative of the generalization gradient across people and, in some cases, setting.
- Caregivers’ proficiency in data collection is assessed using Interobserver Agreement data (IOA), and they are allowed to collect data on their own. Further assistance would be offered in the display and interpretation of the data.
- Caregivers record data on the client’s performance, forwarding the video file to either the BCBA or BCaBA for assessment/evaluation.
This process could be repeated until caregivers reach mastery criteria. It is understood that extraneous variables might play a role in the repetition of the procedure. It is recommended that graphs of the clients—where progress on target behaviors were initially displayed—include probe data points that reflect the generalization assessment.
Many ways are available for making our development a more versatile and adaptable one, and we hope this post serves as the beginning of many ideas to come in the great realm of generalization! Because ABA supports its claims on data, check out our next post on this “Generalization in Times of Crisis” series, which will include data obtained from a survey on telehealth and generalization!

Behavior Analysis Essentials
This entry-level course prepares students to apply the fundamentals of behavior analysis in diverse settings. The training is appropriate for parents, teachers, direct-care staff, and individuals working with persons with autism or developmental disabilities.